How does hypernatremia cause cellular dehydration?
By Sarah Oconnor
How does hypernatremia cause cellular dehydration?
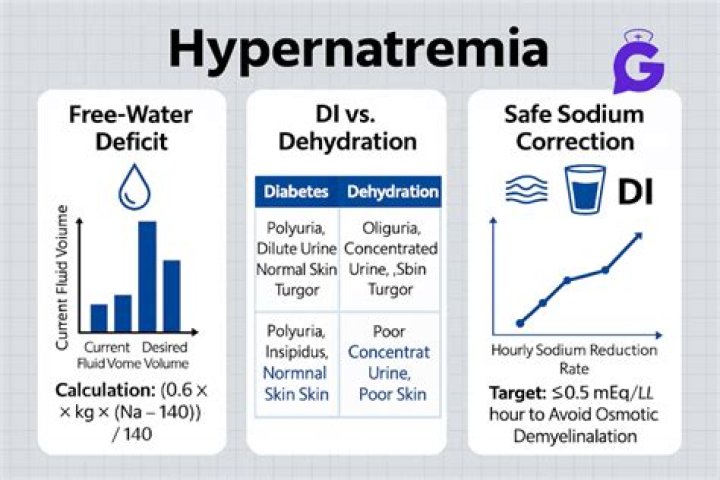
When hypernatremia (of any etiology) occurs, cells become dehydrated. Either the osmotic load of the increased sodium acts to extract water from the cells or a portion of the burden of the body’s free water deficit is borne by the cell.
What causes Hyponatremic dehydration?
Hyponatremic dehydration with a sodium concentration of less than 130 mEq/L (130 mmol/L) occurs when diarrheal losses are replaced with hypotonic fluids. With solute and water loss, ADH is secreted, triggering the body to enhance water absorption.
How does dehydration affect sodium levels?
Chronic, severe vomiting or diarrhea and other causes of dehydration. This causes your body to lose electrolytes, such as sodium, and also increases ADH levels. Drinking too much water. Drinking excessive amounts of water can cause low sodium by overwhelming the kidneys’ ability to excrete water.
Can you be Hyponatremic dehydrated?
Patients may complain of headache, nausea and vomiting, lethargy, and confusion. If the sodium concentration drops quickly to critical levels, seizures, coma, and death may occur. If dehydration is associated with hyponatremia, weakness and muscle aches and cramps may co-exist.
What are some causes of hypernatremia?
Two common causes of hypernatremia are insufficient fluid intake and too much water loss. In rare cases, consuming too much sodium can cause hypernatremia to occur. The opposite of hypernatremia is hyponatremia. This condition occurs when a person’s serum sodium level is less than 135 mEq/l.
How does Di cause hypernatremia?
Extreme dehydration can lead to hypernatremia, a condition in which the sodium concentration of the serum in the blood becomes very high due to low water retention. The cells of the body also lose water.
Does dehydration cause hypernatremia or hyponatremia?
If the balance of fluids and sodium is upset, you can experience hypernatremia – having too much sodium and not enough fluid. Or you can experience hyponatremia – having too much fluid and not enough sodium. Both of these conditions can be the result of dehydration.
What are the causes of hypernatremia and hyponatremia?
Does dehydration cause hyponatremia or hypernatremia?
What is the most common cause for hypernatremia?
Inadequate intake of free water associated with total body sodium depletion. Typically in elderly or otherwise disabled patients who are unable to take in water as their thirst dictates and also are sodium depleted. This is the most common cause of hypernatremia.
How do you correct hypernatremia dehydration?
The most cautious approach is to plan a slow correction of the fluid deficit over 48 hours. Following adequate intravascular volume expansion, rehydration fluids should be initiated with 5% dextrose in 0.9% sodium chloride. Serum sodium levels should be assessed every 2-4 hours.
What is the difference between hyponatremia and dehydration?
Hypernatremia is a condition that occurs due to dehydration (low levels of body water) and an imbalance in electrolytes, including sodium and potassium. A key difference between hypernatremia and common dehydration is who these problems usually affect.
How do you treat hypernatremia?
Hypernatremia is treated with infusions of a solution of water containing 0.9% sodium chloride (0.9 grams NaCl /100 ml water), which is the normal concentration of sodium chloride in the blood plasma. The infusion is performed over many hours or days to prevent abrupt and dangerous changes in brain cell volume.
What is the best way to cure dehydration?
Water is the best way to prevent and beat dehydration, especially during the warm summer months when we’re all prone to perspiring even more than usual. Simply consuming the recommended eight to 10 eight-ounce glasses of water on a daily basis is usually enough for most to maintain healthy electrolyte levels.
What IV fluids are given for hypernatremia?
In patients with hypernatremia and hypovolemia, particularly in patients with diabetes with nonketotic hyperglycemic coma, 0.45% saline can be given as an alternative to a combination of 0.9% normal saline and 5% D/W to replenish sodium and free water.